7 Critical Tests Your Shoulder Physio Specialist Performs
Jump To Key Section

“Take care of your body. It’s the only place you have to live.”
– Jim Rohn (Entrepreneur & Author)
Shoulder pain can turn your day-to-day tasks into frustrating challenges. It becomes difficult to reach for a shelf, lift groceries, or get dressed. Because it’s the body’s most mobile joint, pinpointing the exact source of pain isn’t always straightforward. That’s why shoulder physiotherapists rely on a series of specialised clinical tests instead of guesswork.
A comprehensive physical examination and assessments help identi y muscles, tendons, or ligaments responsible for the painful symptoms. Here are the seven key tests your shoulder physio specialist performs to accurately diagnose your condition and create a personalised recovery plan.
KEY TAKEAWAYS
- Shoulder physiotherapists use multiple clinical tests to accurately diagnose the source of pain rather than relying on symptoms alone.
- Different tests assess specific structures, including the rotator cuff, biceps tendon, and ligaments.
- Identifying the exact cause of shoulder pain leads to a more targeted and effective rehabilitation plan.
- Early assessment can help prevent ongoing pain, reduced mobility, and further damage
1. Neer’s Impingement Test
The Neer Impingement Test helps determine whether your rotator cuff tendons are being compressed beneath the bony arch of your shoulder. It’s a common cause of persistent pain. During this assessment, your provider will stabilise your shoulder blade with one hand while gently raising your fully extended arm right next to your ear. If you feel this sharp, familiar pain during this upward motion, you likely have structural impingement.
A shoulder physio in Fitzroy will help you deal with pain because they will use this test along with other movements to check the health of your joints. This detailed physical assessment ensures that your treatment programme directly addresses the appropriate anatomical structure.
2. Empty Can (Jobe) Assessment
Empty Can test checks the condition and health of your supraspinatus muscle. You will be instructed to lift your arms forward at an angle, turning your thumbs downward as if to empty a water bottle. The expert will then gently press some force downwards on your arms, and you’ll actively resist it.
If there’s noticeable weakness or sharp pain resisting the downward pressure, it’s either a supraspinatus tendon tear or significant inflammation. It provides immediate, invaluable data about your muscle’s true load-bearing capacity.
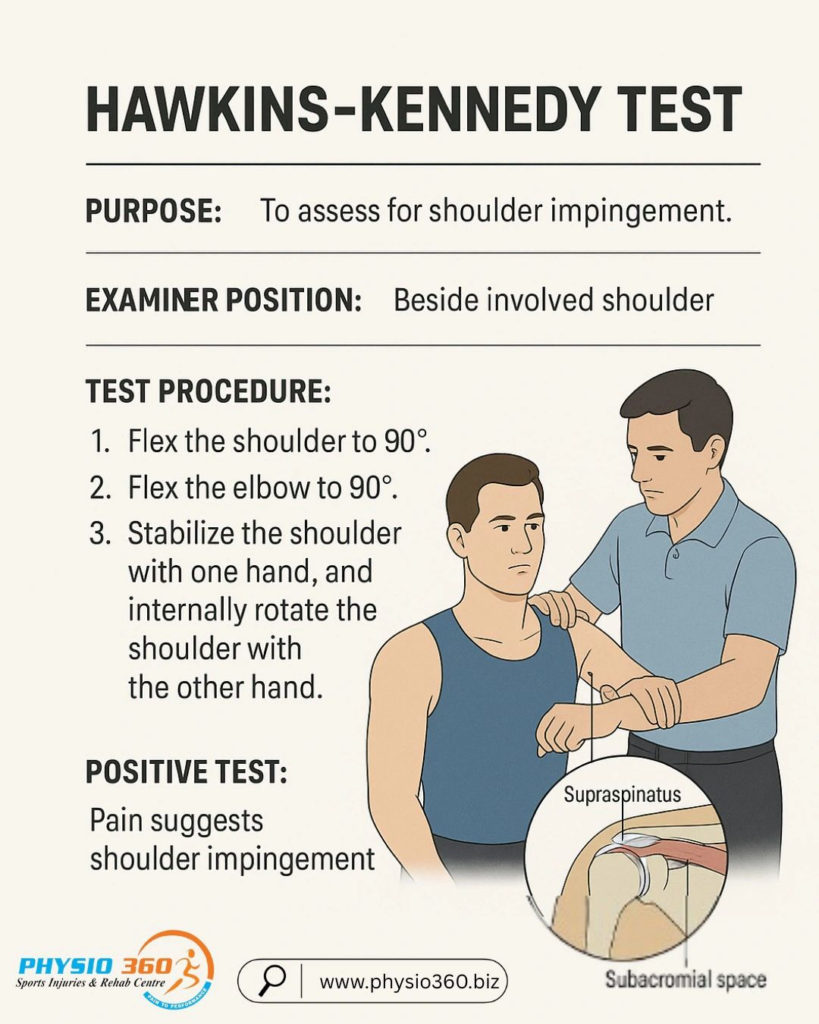
3. Hawkins-Kennedy Compression Test
The Hawkins-Kennedy test tests a different area of the shoulder joint. Your therapist will flex your elbow to a ninety-degree angle and elevate your upper arm forward, parallel to the floor. From this baseline position, they will quickly turn your forearm downward to compress your internal tendons.
If this internal rotation produces a painful feeling deep within the joint, it shows that your soft tissues are trapped and inflamed. This important piece of clinical information helps your therapist evaluate potential causes of your daily discomfort.
4. Apprehension and Relocation Test
For athletes who have suffered a prior shoulder dislocation or subluxation, it is imperative not to neglect the assessment of joint stability. Your therapist will place your arm out to the side so that you can carefully rotate your forearm backwards to test the structural boundaries of the joint. They observe your facial expressions and muscle response for physical signs of anxiety or structural slipping.
If they immediately apply a stabilising force to the front of the joint and your pain goes away, the relocation test was successful. Such a result clearly highlights anterior joint instability, which needs to be addressed through targeted strengthening.
5. Speed’s Test for Biceps Tendonitis
The rotator cuff isn’t related to all pain situations. It can actually be within the long head of your biceps tendon. To assess for this, you will extend your arm straight out in front of you with your palm facing directly up towards the ceiling.
As you work to maintain a perfectly level arm, the clinician will apply a downward force against your forearm. Feeling a distinct, localised pain right along the front groove of your shoulder indicates significant biceps tendonitis or a potential labral tear.
6. Lift-Off Test for Subscapularis Health
The subscapularis is a large, powerful muscle found at the front of your shoulder blade that is notoriously difficult to isolate and test. To evaluate it, place the back of your hand directly against your lower spine and try to push the hand away from your body. Your specialist will provide resistance to this backward movement to measure your muscle recruitment.
If you cannot lift your hand off your lower back or have a total lack of strength, it indicates a strain or tear of the subscapularis. Uncovering this hidden weakness is absolutely vital for restoring your arm’s natural internal rotation capabilities.
7. Sulcus Sign Test for Multi-Directional Laxity
When you are totally relaxed while sitting, the expert will hold your forearm and apply a gentle downward tug towards the floor. They carefully observe the top of your shoulder joint, looking for a small, visible dimple or gap beneath the bone.
A prominent gap indicates the ligaments around the bone are too loose and are unable to keep the arm bone tightly in place. It’s a great piece of evidence that tells your therapist to plan a lot more for joint stabilisation than for muscle stretching.
Mapping Your Personal Recovery Journey
These seven clinical tests provide valuable insights into the functioning of your shoulder and what’s causing the pain. Your physical therapist may use this checklist to safely get your joints working again. If you know exactly which muscles, tendons, or ligaments are holding you back, you won’t have to make the misguided guesses that come with recovering from an injury.
Never let chronic shoulder discomfort keep you from your daily physical independence. To make that right, a specialised practitioner will work with you so you get an accurate diagnosis, a targeted plan for recovery, and a confident return to those activities you love.
FAQs
Ans: No single test can diagnose for every condition. Performing multiple assessments allows the physiotherapist to evaluate different muscles, tendons, and ligaments before reaching an accurate diagnosis.
Ans: Most tests cause only mild discomfort if the injured structure is involved. Your physiotherapist performs each movement carefully and will stop if the pain becomes excessive.
Ans: Clinical tests can strongly indicate a rotator cuff injury, but imaging such as an ultrasound or MRI may be recommended to confirm the diagnosis when necessary.